
The ageing of the population is one of the great challenges that societies will face - and are facing - in the 21st century. One fact: in 1950 only one in every hundred people on the planet was over 80; in 2050, one hundred years later, estimates indicate that ten out of every hundred people will be over 80 in OECD countries. This change in the demographic structure has numerous social and economic implications: how will it affect consumption, investment and savings patterns? How will it affect public finances and administrations? How will it alter care relationships or our understanding of care? How will it affect families? Socio-economic structures influence how individuals are constructed in society, so how profound will this material change be and how will it alter social subjects? The possibility of responding to this challenge is also a valuable source of opportunity.
The way of understanding ageing, how to grow old and the social policies that allow people to live better in advanced ages must evolve, adapting to future needs with a clear purpose: to avoid the unsustainability of the system, the loss of care quality when dependency arises and, above all, to avoid the fatal scenario in which the absence of care leads to neglect or even abandonment. However, not all states will face these changes in the same way since, in turn, the material conditions of these states are determined by their own social, economic and political history. For this reason, in this entry we are going to review some concepts of care systems because by understanding them better we will be able to develop better public policies.
The care diamond
A system is, according to the SAR, a "set of things which in an orderly fashion contribute to a certain object". The organization of care in a society behaves in a systemic manner, since the set of elements that make it up contributes to an object: care. As Shahra Razavi explains, every welfare regime has a care regime. Based on Esping-Andersen's approach, there is a "welfare triangle" formed by the State, the market and families, and this same triangle would be applicable to the care system. A system with low state intervention would give the market full control over how, where, who and at what price services will be provided. This could overburden the most disadvantaged families and increase the inequality gap in our societies. High intervention could partially - or totally - unburden families, but it could drive the market out of the system and this could overburden the public benefit system. However, this triangle would be leaving aside a sector that has traditionally also supported part of the long-term care system: the voluntary and non-profit sectors. These organisations have been - and are - important. For example, in developing countries - and also in some developed countries - minimum care services for the elderly, orphans and the chronically ill are provided through charitable, religious and community organizations. Adding the non-profit sector to Esping-Andersen's initial approach would transform the initial triangle into a diamond: a care diamond (Figure 1).
Figure 1. Care diamond
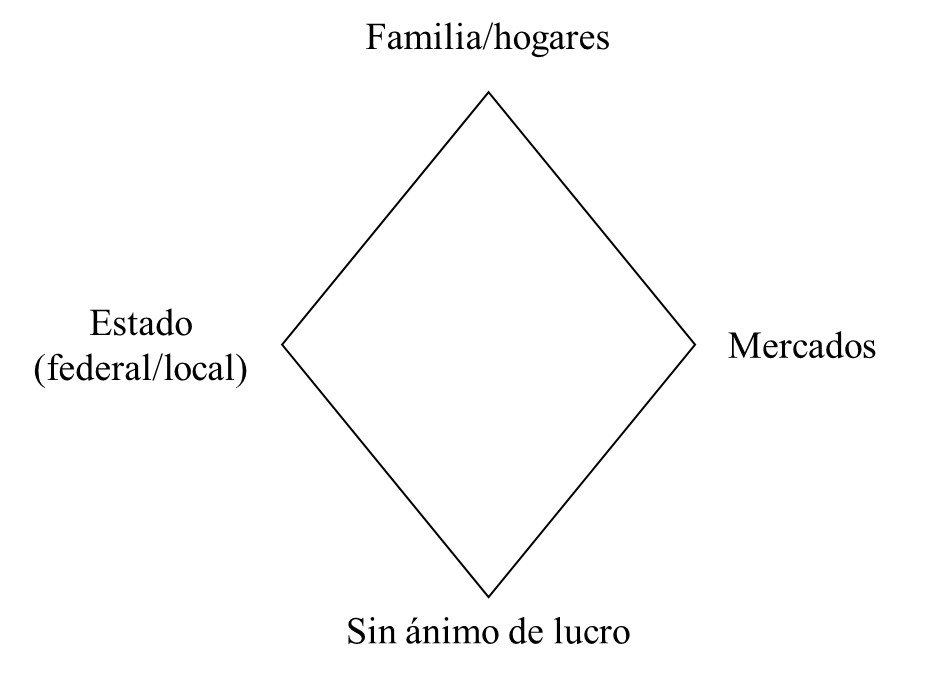
Source: Translated of Razavi (2007)
The role of the state in this care diamond is therefore very important. First, because it protects families by providing services, but also, depending on the policies it develops within the family, the burden of care among the groups that make up the system may vary considerably. And this is crucial.
The distribution of the diamond: shared, semi-shared and non-shared systems
Jesús Rogero-García uses the care diamond metaphor to theoretically propose three types of systems based on how care is divided among the four agents - State, market, family and non-profit sector. He thus identifies three types of systems (Figure 2): shared, semi-shared and non-shared. The diamond represents the needs of the dependent people and the circles around the diamond represent the agents. The size of the circle indicates the weight that these agents have in each society. Their presence - or absence - in the diamond is the agent's contribution to meeting the needs of dependants.
Figure 2. The three systems of care for dependent persons: shared, semi-shared and non-shared

Source: Translated of Rogero-García (2012)
The evolution of the systems begins with a non-shared system in which all care is family, private - demanded by the wealthiest families - and mainly female. The public sector is not involved in the provision of services. As the region develops, it evolves into a semi-shared system where the family burden is slightly reduced and the State and markets begin to participate in service provision. This system arises when the Welfare State begins to be implemented and governments begin to consider problems linked to dependency as a social risk. The shared system is, therefore, the evolution of the semi-shared system, in which family burdens try to be reduced, the State continues to cover needs and the market begins to see a clearer business opportunity in people's dependence. The shared system operates, for example, in most European countries, North America, Japan or Australia. Semi-sharing would fit in Latin America and Asia - although it may also appear in some European countries. The non-shared would be found in Africa. The main coincidence between the diamonds in each system is the great weight borne by the family, and the secondary one is that non-profit organisations maintain a similar weight in any of the systems -their weight is small, but necessary when there are material shortages.
However, several of these systems may coexist in the same country or region. For example, in Europe we can find, among others, the Nordic model, the Anglo-Saxon model, the Mediterranean model and the continental model. At the same time, these models are subject to change due to variations in state and regional policies. In general, in Europe, in the 1990s, care expanded, risk was understood as a social problem, services were provided. From 2000 onwards, attempts were made to rationalise and contain the cost, risk was re-familiarised and individualised, and cash benefits were promoted. These latest changes, marked by budgetary constraints, follow the criteria governing the economy established in the West and may lead to the risk of dependency being individualized, no longer considered a social problem but a particular one. This would again alter care systems. The shared system presented here has therefore been evolving towards a shared, neo-liberal system in which the State has less and less weight -due to cost containment-, families regain the traditional family burden of care, and whoever needs care must cover their risk individually -either through private insurance, relying on the family, or with their savings. But is this alternative the most appropriate?
People who can save or afford private insurance will have no problem; the problems will be faced by those who, due to different circumstances, cannot save, have support networks or afford such insurance. Those people, those families, will be in a situation close to social exclusion. Therefore, if these policies were to evolve into New-Keynesian-style policies in which the State intervenes to guarantee equity and efficiency, these families would be better off and could continue to participate in the economy, eliminating - or considerably reducing - the possibility of entering into a risk of social exclusion (Figure 3). This would form the New-Keynesian shared system.
Note to the reader: This entry is based on a paper co-written by Isabel Pardo García and Roberto Martínez Lacoba that was presented at the XII International Conference on Economic Policy, held in Toledo on 28-29 May 2015. You can access to its complete reading through this link.
Figure 3. Evolution of long-term care systems
Source: Own elaboration
The current system, which we have called the shared neo-liberal system, has evolved to help the most serious cases, but there are situations of dependency that are not covered - let us also think about child care. We need policies that enable us to reconcile working life with care and that do not place it on women. If the State does not intervene to guarantee the protection of families and ensure equity among their inhabitants, the problem of dependency will worsen. In that case -that of non-intervention due to pressures of different nature-, a spiral of destruction of well-being could begin from which it will be difficult to escape, disrupting families, reducing the number of people in the labour market because of the need to care, and possibly affecting negatively the income of the administrations. In a scenario that is difficult to imagine, almost apocalyptic, but -why not?- possible, the dependent person could have to go into exile from society as we know it today. And these scenarios should not be considered. That is why we must first find a sustainable, equitable, efficient and also flexible solution in the medium and long term for care systems: inclusive systems that do not allow any citizen to fall into neglect.

