
Care is the support or assistance provided to people in need. The RAE defines care, in its second sense, as "To assist, to keep, to preserve. To take care of a sick person, the house, the clothes". In its first meaning, which would complement the previous one if we speak not only of care, but of quality care, the RAE establishes care as "To put diligence, attention and request in the execution of something".
We understand that the potential demanders and receivers of this care would be children, the elderly and dependent people in general. In other words, people who need the care. However, we can all be recipients of forms of care at different times in our lives, even if we do not fit a priori in the definition of dependents or we have stopped needing assistance strictly. For example, we receive care when we are ill. But also at other times when there is no real need, such as when we go from "table to table" visit to the grandmother's house and we take four tápers with us. I conceive care in a broad way, referring to all those attentions that facilitate our life so much and that are not remunerated in any way.
That is to say, without needing assistance we can be daily recipients of care tasks that make our daily life easier. These small forms of care (such as tápers) are often overlooked (despite the enormous impact they have on the quality of our lives) but, to a large extent, large manifestations of care also seem to lack prestige.
Care has traditionally been discredited and considered completely separate from productive work. And this has a terrible consequence on the care itself, making invisible the effort of the caregiver, but also assuming the quality of the care emitted and the capacity of the caregiver. As far as care is concerned, and unlike other activities that are not so fundamental to the maintenance of human life and well-being, there is a tendency to assume that anyone, by the mere fact of wanting or (worse) having time or not having a recognized productive activity (i.e. not charging) can do so. And that, in addition, he will do it well.
This is an issue that should be of great concern to us. But there are others to think about.
A few days ago I published this article on the overload of care in the home and the outsourcing of the same through the hiring of domestic service, which would be another option other than the one we are talking about today. What I pointed out in that article is how social and demographic changes (less caregivers for a greater number of caregivers) produce an enormously difficult situation, which does not find optimal solutions either from the private or from the public. This difficulty would point to three issues: the overload of the family, which cannot respond to the growing need for care; the lack of adequate and sufficient public responses on the part of the State; and finally, the regulation of domestic service, which plunges workers into situations of vulnerability, demonstrating the low social value of care in today's society (without this meaning that in the past it was better valued). With regard to the first point, in addition to the family overload, which cannot cover the need for care due to time constraints, it is necessary to reconsider whether it is capable of providing quality care.
As we have pointed out on other occasions, the increase in life expectancy (in 2016 Eurostat points out that Spanish women are the longest in Europe, with 86.3 years and men the seventh, with 80.5 years) leads to a greater need for care, which is not necessarily true, or at least not in a simplistic way. More people reach longer ages, which means there are more potential caregivers. But, in addition, and this would be the important part, when we need care, we need it for longer (because even affected by disease, life expectancy is still longer). In relation to this issue, here appears something that is fundamental to me and that we would need to reflect on when approaching care from the Welfare State: this greater survival also occurs in people who suffer from disability and / or chronic diseases, increasing the complexity of the care they need. Nevertheless, it is still assumed that the ability to take care (and to do it well) depends on will and is related in the imaginary to the love one has for those in need of care. And that sometimes leads to strenuous efforts to provide that care to loved ones. This is consistent with a generalised preference in Spain, as opposed to other European countries, for care by families or co-residency (living with one of the children who would be providing the care):
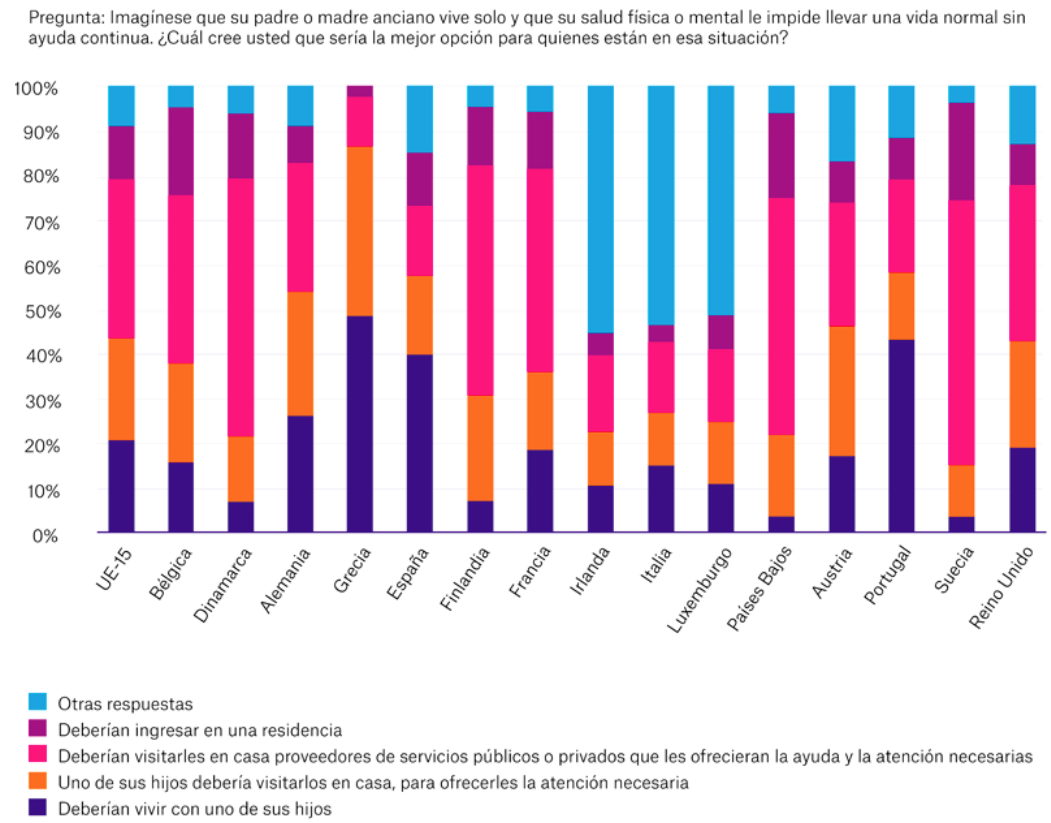
Source: Costa-Font (2017).
I do not doubt the enormous good will of the sons (daughters, we are not going to deceive ourselves, that although the care of childhood seems to begin to change, the care of elderly dependents continues in the hands, full to overflowing, of the women) but I do doubt more of the capacity and the knowledge to be able to provide the necessary care that allow to speak of an aging of quality.
But there is also a fundamental question that has perhaps not been given enough thought: the longer life expectancy in health means that the need for care associated with old age is delayed. But this also means that the caregivers (daughters, daughters-in-law) are also older when they have to start caring. Above all, by increasing life expectancy in a situation of dependency, care is issued for a longer period of time. Finally, this means that we are carers until later ages, and sometimes the need for our own care may overlap with the care issued. And here is the question: Can I give care or do I need it? Is who has become in need of care giving care? When this happens, and it happens to a greater and greater extent, not only are we hindering autonomy in old age and overburdening carers, but inevitably the quality of care and therefore the quality of life of both parts will be diminished.

